So you have a disc bulge…., what does it mean for you?

If you have had back pain for a while, it is likely someone has ordered imaging of your back. Typically, the report will report all sorts of findings. Many of these findings are present without causing symptoms. Often one or more lumbar discs are reported as “bulging”. Maybe you were told you had a bulging disc and now you are concerned with what this might mean for you. So, read on….., this primer will give you an overview on understanding disc injuries. (There are supporting research references if you really want to dig deeper).
INSIGHT: A major consideration in the discussion of disc injuries, is to ask why your back pain is present (or “why do I have a disc injury”). Keep in mind that focussing on a disc injury is only part of the process of understanding why you have back or neck pain. Identifying movement, posture, strength and overloading issues are the main areas that drive treatment strategies and recovery, including when discs are “bulging”.
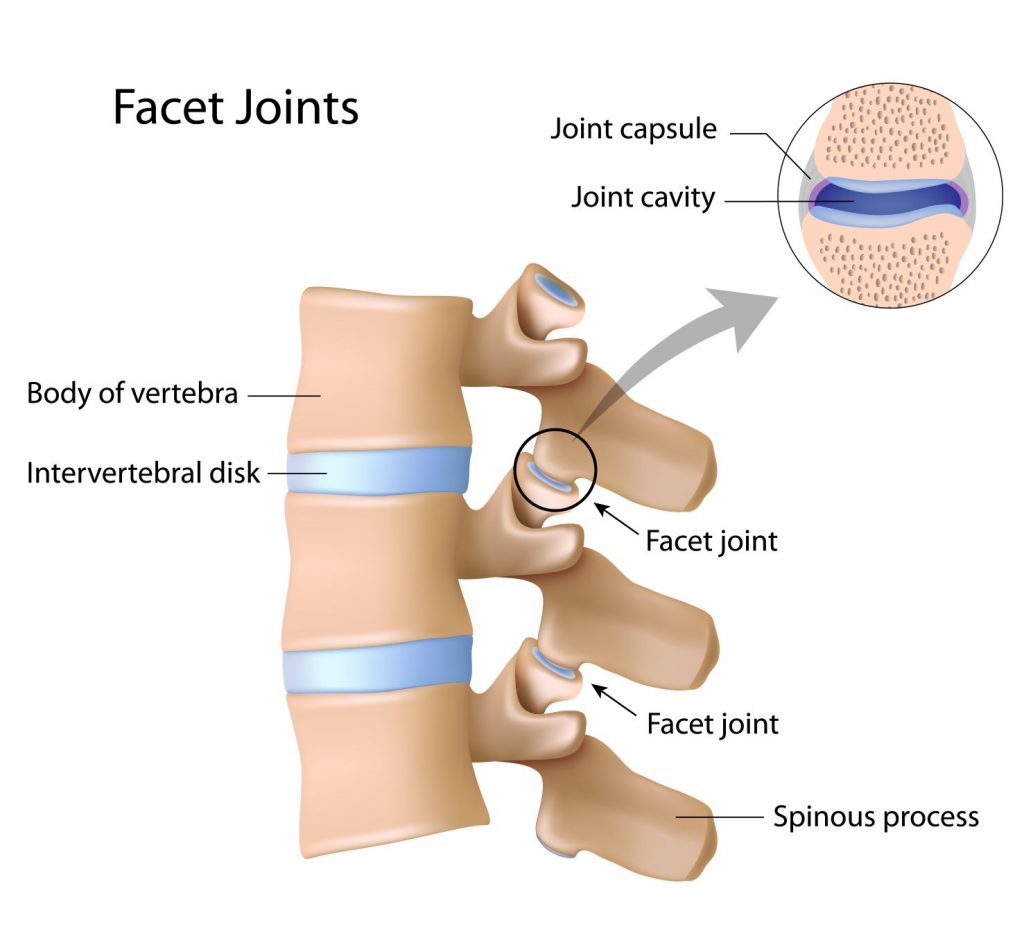
Firstly, lets’ start with the ‘language’ of disc injuries. Terms like disc herniation and disc prolapse are generic terms that cover all disc injuries. A more exact method of describing disc injuries is to classify them into three main types; bulges, protrusions and extrusions. Each type of disc injury has a wide range of clinical implications that vary all the way from ‘no effect on you’ to the need for surgery. I’ll describe each type of disc injury below. But firstly, understanding the basic anatomy is helpful. The image below will show you the basic structure and terminology.
Disc bulges
Disc bulges are the most common finding seen on imaging. They are are commonly found in people with and without back pain. Some people who are known to have disc bulges have never experienced back pain. A disc bulge might be associated with pain but this will depend a number of things such as if a sudden tear has occurred, if there is inflammation, if the bulge combines with other components to narrow spaces for nerves, if there is damage to the ‘endplates’ that are on the top and bottom of the disc etc. It’s important to understand that pain intensity does not directly relate to the size of the bulge. This means that you could have strong pain with only a minor disc bulge.
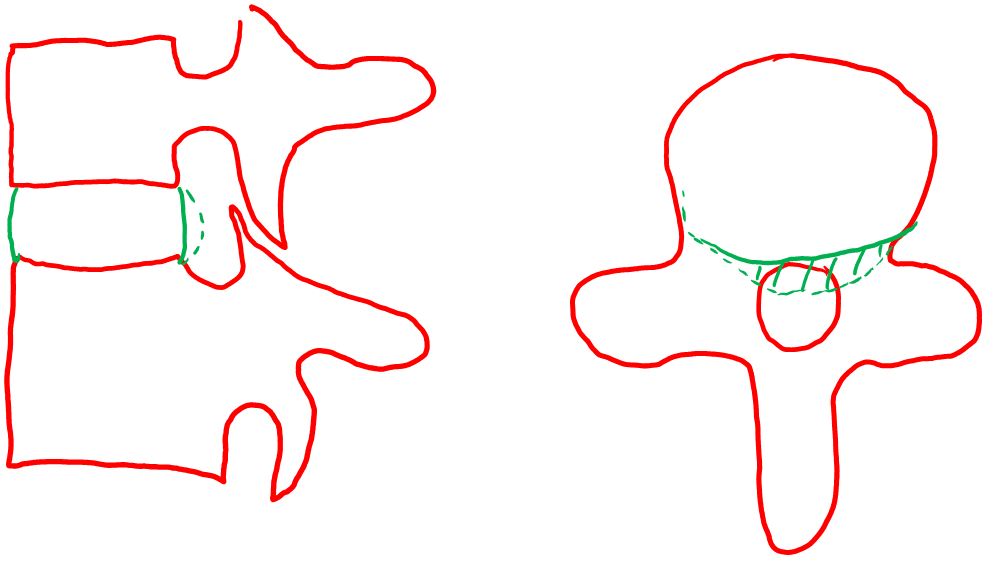
This image illustrates a typical disc bulge, that is broad-based and usually does not cause nerve compression.
Annular tears
Small disruptions to the outer fibrous ring of the intervertebral disc (known as the the annulus fibrous) can occur and these are called ‘annular tears’. They can be present with or without pain and do not require surgical intervention. Annular tears may be associated with pain and annecdotally, seem to take several weeks to settle. During the recovery time it is not uncommon to have flare-ups of pain followed by further recovery. The two images below show small white (bright) areas at the back of the disc that indicate annular tears.
Disc protrusions
Disc protrusions are asymmetrical disc bulges that usually affect one side of the disc, with the possibility (but not always) of compressing nerve tissue. People often describe their pain as a “pinched nerve” but true symptoms of nerve compression include sensory changes such as ‘pins and needles’ (paraesthesia) or numbness (anaesthesia), loss of strength and reduced reflexes. Pain is often present but pain alone does not always indicate nerve entrapment.

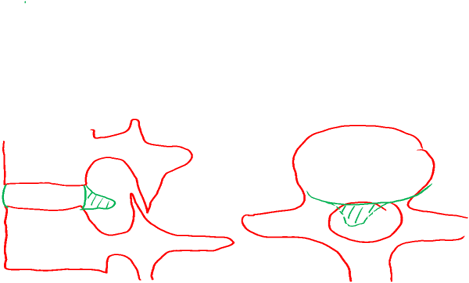
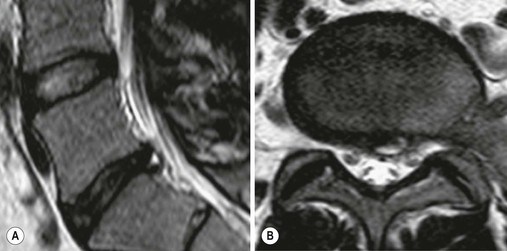
This image and the line drawing illustrate a disc protrusion when looking from side on (sagittal view) or from above or underneath (axial view).
Disc extrusions
A disc extrusion occurs with a tear in the annulus that allows gel-like material to emerge from the disc, similar to a disc protrusion but with the disc material extending vertically past the upper or lower endplate of the vertebrae. Extrusions may extend in any direction, and can be quite large. If the extrusion is directly in the midline it may not cause nerve compression but if it occurs either side of midline nerve compression may occur. The nerve that is getting ready to exit the spinal canal (the traversing nerve) can be compressed in the region known as the lateral recess (in the posterolateral aspect of the spinal canal). In recent studies, extrusions were more commonly associated with signs of nerve root compression (often know as a radiculopathy).
However, disc extrusions are an example of size not meaning everything. A number of studies have shown that large disc extrusions shrink (regress) over time. Some types of disc injuries such as protruded and extruded discs may do better with surgical decompression, but the natural history of recovery will mean that many people with significant disc injuries do not need surgery.

Disc extrusions can ascend or descend as shown in this image.
Recovering from a disc injury
As a general rule, recovery strategies will include activity and movement while respecting nerve sensitivity. Typically, many people show slow but steady recovery over a three month period. Some people who have significant nerve damage, high levels of pain and/or slow recovery may require earlier surgical intervention. Physiotherapy, exercise and gradual return to activity are usual first line strategies of management.
References for further reading:
- Ahn, T.-J., et al. (2009). “Effect of intervertebral disk degeneration on spinal stenosis during magnetic resonance imaging with axial loading.” Neurologia Medico-Chirurgica 49(6): 242-247; discussion 247.
- Allan, G. M., Spooner, G. R., & Ivers, N. (2012). X-ray scans for nonspecific low back pain: A nonspecific pain? Canadian Family Physician, 58(3), 275.
- Ammendolia, C. and N. Chow (2015). “Clinical outcomes for neurogenic claudication using a multimodal program for lumbar spinal stenosis: a retrospective study.” Journal of Manipulative & Physiological Therapeutics 38(3): 188-194.
- Ammendolia, C., et al. (2014). “What interventions improve walking ability in neurogenic claudication with lumbar spinal stenosis? A systematic review.” European Spine Journal 23(6): 1282-1301.
- Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects: a prospective investigation. J Bone Joint Surg Am 1990;72:403–8.
- Brinjikji, W., et al. (2015). “MRI Findings of Disc Degeneration are More Prevalent in Adults with Low Back Pain than in Asymptomatic Controls: A Systematic Review and Meta-Analysis.” American Journal of Neuroradiology 36(12): 2394-2399.
- Endean, A., et al. (2011). “Potential of Magnetic Resonance Imaging findings to refine case definition for mechanical low back pain in epidemiological studies.” Spine 36(2): 160-169.
- Fardon et al American Spine Society ASoSR, American Society of N (2001) Nomenclature and classification of lumbar disc pathology. Recommendations of the Combined task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine 26:E93–E113
- Fardon, D. F., et al. (2014). “Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology.” The Spine Journal 14(11): 2525-2545.
- Gilbert, J. W., et al. (2008). “Imaging in the position that causes pain.” Surgical Neurology 69(5): 463-465.
- Gilbert, J. W., et al. (2010). “Lumbar disk protrusion rates of symptomatic patients using magnetic resonance imaging.” Journal of Manipulative and Physiological Therapeutics 33(8): 626-629.
- Graves, J., et al. (2012). “Early Imaging for Acute Low Back Pain.” Spine 37(18): 1617-1627.
- Hancock, M. J. P., et al. (2017). “Is the Number of Different MRI Findings More Strongly Associated With Low Back Pain Than Single MRI Findings?” Spine 42(17): 1283-1288.
- Hancock, M., et al. (2015). “Risk factors for a recurrence of low back pain.” The Spine Journal 15: 2360-2368.
- Henschke, N., et al. (2013). “Red flags to screen for malignancy in patients with low-back pain.” Cochrane Database of Systematic Reviews(2).
- http://www.sahealth.sa.gov.au/wps/wcm/connect/bc896c004a59dcf8b02df07633bbffe0/ImagingGuideline-RAH-AlliedHealth-1201023.pdf?MOD=AJPERES&CACHEID=bc896c004a59dcf8b02df07633bbffe0
- Jarvik, J. J., et al. (2001). “The Longitudinal Assessment of Imaging and Disability of the Back (LAIDBack) Study: baseline data.” Spine 26(10): 1158-1166.
- Jensen M, Brant-Zawadzki M, Obuchowski N, Modic M, Malkasian D, Ross J. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 1994;331: 69–73.
- Jensen, T. S., et al. (2006). “Natural course of disc morphology in patients with sciatica: an MRI study using a standardized qualitative classification system.” Spine 31(14): 1605-1612; discussion 1613.
- Manchikanti, L., et al. (2015). “A Systematic Review and Best Evidence Synthesis of the Effectiveness of Therapeutic Facet Joint Interventions in Managing Chronic Spinal Pain.” Pain Physician 18(4): E535-582.
- Manchikanti, L., et al. (2016). “Utilization of Facet Joint and Sacroiliac Joint Interventions in Medicare Population from 2000 to 2014: Explosive Growth Continues!” Current Pain & Headache Reports 20(10): 58.
- National Institute for Health and Care excellence (NICE) Guidelines 2016-17 https://www.nice.org.uk/guidance/qs155/chapter/Quality-statement-2-Referrals-for-imaging
- Ohtori, S., et al. (2015). “Pathomechanisms of discogenic low back pain in humans and animal models.” The Spine Journal 15(6): 1347-1355.
- Peng, B., et al. (2006). “The pathogenesis and clinical significance of a high-intensity zone (HIZ) of lumbar intervertebral disc on MR imaging in the patient with discogenic low back pain.” European Spine Journal 15(5): 583-587.
- Perez, A., et al. (2007). “Evaluation of intervertebral disc herniation and hypermobile intersegmental instability in symptomatic adult patients undergoing recumbent and upright MRI of the cervical or lumbosacral spines.” European Journal of Radiology 62: 444-448.
- Pfirrmann, Metzdorf, et al. (2001). “Magnetic Resonance Classification of Lumbar Intervertebral Disc Degeneration.” Spine 26 (17): 1873-1878.
- Raastad, J., et al. (2015). “The association between lumbar spine radiographic features and low back pain: A systematic review and meta-analysis.” Seminars in arthritis and rheumatism 44: 571-585.
- Sheehan, N. J. (2010). “Magnetic resonance imaging for low back pain: indications and limitations.” Ann Rheum Dis 69: 7-11.
- Sizer, P et al. (2007). “Medical Screening for Red Flags in the Diagnosis and Management of Musculoskeletal Spine Pain.” Pain Practice 7(1): 53.
- Teraguchi, M., et al. (2015). “The association of combination of disc degeneration, end plate signal change, and Schmorl node with low back pain in a large population study: the Wakayama Spine Study.” The Spine Journal 15(4): 622-628.
- Webster, B. S. B. P. A., et al. (2014). “The Cascade of Medical Services and Associated Longitudinal Costs due to Non-Adherent MRI for Low Back Pain.” Spine.
- Webster, B., et al. (2013). “Iatrogenic consequences of early magnetic resonance imaging in acute, work-related, disabling low back pain.” Spine 38(22): 1939-1946.
- Zehra, U., et al. (2017). “Defects of the vertebral end plate: implications for disc degeneration depend on size.” The Spine Journal 17: 727-737.